At AcademyHealth's recent National Health Policy Conference, noted geriatrician Joanne Lynn, MD began her session on end-of-life care by asking for a show of hands. How many of you want to grow old? All hands are raised. How many of you expect to die? Nervous laughter, as almost all hands are raised again. Then she gave us a few choices about how we might want to die. How many of you would choose cancer? Almost no one. How many would choose heart or lung disease? Only a smattering of hands. Okay then, Dr. Lynn concluded, "you're all hoping for frailty."
If we live until 75, Dr. Lynn explained, we are likely to live many years needing assistance with two or more activities of daily living (ADLs). She
Janet Weiner, MPH, is Associate Director for Health Policy at the University of Pennsylvania's Leonard Davis Institute of Health Economics (LDI) and editor of the LDI Blog.
and her panelists described a health care system woefully unprepared to meet the needs of a growing frail elderly population, who often need basic support services such as meals, transportation, or respite care.
Lack of funding There is little funding for services that could keep people out of the most expensive long-term care settings (nursing homes) and in their homes, where most prefer to be. "I can write a prescription for the most expensive drug and Medicare will pay for it, but I can't write a prescription for food," Dr. Lynn said.
Lisa Shugarman, PhD, Director of Policy for the SCAN Foundation, drove home the following messages: first, that end-of life-care is more about living with advanced disability than about dying; second, that it is about function, not just disease; and third, that making no changes to our present system is the most expensive option.
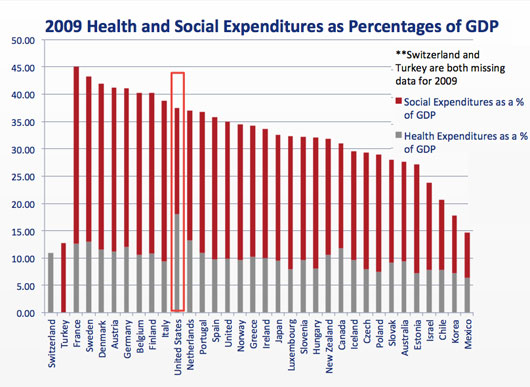
Low social spending She and other panelists noted that the U.S. matches its high spending on health care with remarkably low spending on social supports, as shown in these charts from the OECD Health Data 2009. The first chart shows that the U.S. is on par with other developed nations when social and health spending are combined. The U.S spends less of its GDP than France, Denmark, Germany and Finland:
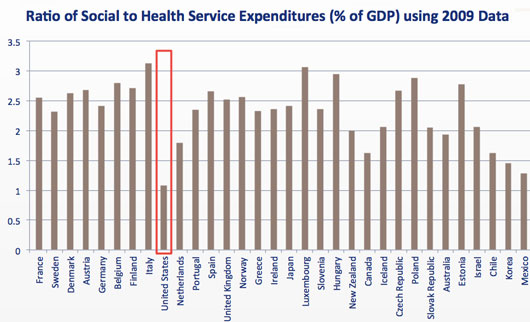
What sets the United States apart, however, is its ratio of social to health spending. Other nations spend two to three times as much on social programs as on health, while the U.S. spends about the same on health as it does on social programs. The panelists suggested that spending in the health care system is crowding out other spending on long-term support services that people need and want:
But the session was far more than a recitation of the problems and challenges of end-of-life care. Panelists described innovative programs being tested and strategies that have worked. The recurrent theme in all of them was a client-centered approach, in which medical and non-medical services are coordinated.
Integrating acute and long-term care Mimi Toomey, Director, Office of Policy Analysis and Development, HHS Administration for Community Living, spoke about her agency's work with state and community-based aging and disability agencies. She described ongoing work with the Centers for Medicare & Medicaid Services (CMS) on integration of acute care and long-term services and supports. For example, the Community-based Care Transitions Program reduces hospital readmissions by providing a broad range of services such as transportation, home-delivered meals, homemaker services, and injury prevention visits.
"We're finding what we've known all along," Toomey said, "that it's really not the medical condition that brings people back to the hospital. You can have a perfect care plan, a perfect discharge plan... only to find out that the person has no food in their refrigerator, and they don't have a ride back to the follow-up physician."
Suzanne Burke, CEO of the Council on Aging of Southwestern Ohio, described the successful model of a non-profit, community-based agency that operates as a single point of contact for regional aging and disability resources. It coordinates and manages long-term care services and supports, and provides community services such as wellness activities, Alzheimer's services, legal help, transportation, and outreach. To keep people in their homes, she noted, "home health is not enough."
Ohio success story Her agency, through Medicaid waivers and a county property tax, provides a broad range of in-home services that allow frail elders to remain in their homes at a fraction of the cost of nursing home care. She also noted that even in an economic downturn, the property tax has passed in five counties because people recognize the program as an essential, shared community resource.
On the legislative front, Elizabeth Falcone, senior advisor to Sen. Mark Warner, described the bipartisan Care Planning Act (S. 1439), a bill introduced last fall by Sen. Warner (D-VA) and Sen. Isakson (R-GA). Targeted to people with advanced illness, "it's designed to align the care they get with care they need," she said. She outlined a number of provisions, including:
Reimbursement under Medicare Part B for creating a planning document with advanced illness goals, values, and preferences
A Center for Medicare and Medicaid Innovation (CMMI) pilot test of advanced care coordination ("hospice lite")
Grants for providers and for public education about advanced illness, and
Development of new quality measures to track whether care is meeting the goals of the individual.
The bill remains in the Senate Finance Committee for consideration.