Clinical Director, William Carey University College of Osteopathic Medicine
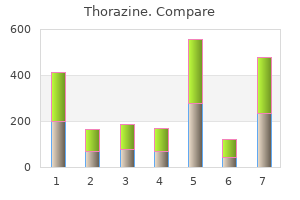
With such a diet it is also difficult to achieve sufficient fiber intake to meet recommendations [1 medicine 1950 buy discount thorazine 100mg line,24 symptoms bipolar disorder cheap 50mg thorazine amex,25] medicine jewelry buy generic thorazine 100 mg online. Having this in mind symptoms 4dp5dt cheap thorazine uk, it does not appear to be productive to overemphasize the present renaissance of low carbohydrate strategies in diabetes. Furthermore, several recent reports on this topic do not clearly define what is meant by "low" or "high" carbohydrate and whether a carbohydrate intake of around 40% of total energy, which is consumed by many people with diabetes, already corresponds to a low carbohydrate diet [26,27]. Glycemic effects of different carbohydrate Not only the amount of carbohydrate, but also the quality of carbohydrate is important for individuals with diabetes. Vegetables, legumes, fresh fruit, wholegrain foods and low fat milk products should be part of a healthy diet [1,2]. South (n = 1371) Total energy (kcal/day)a Carbohydrate (% of energy) Fiber (g/day)a Total fat (% of energy) Saturated fatty acids (% of energy) Cholesterol (mg/day)a Protein (% of energy) Alcohol (g/day)b Current smokers (n %) Ex-smokers (n %) Vigorous exercise once/week (n %) 2148 43. Southern European Centers (n = 12): Athens, Bari, Cagliary, Lisbon, Milan, Padua, Perugia, Pisa, Rome, Turin, Thessaloniki, Verona. Northwestern European Centers (n = 15): Cork, Dьsseldorf (two centres), Gent, Helsinki, Leiden, London, Luxembourg, Manchester, Munich, Paris, Sheffield, Valenciennes, Vienna, Wolverhampton. In the process of achieving desirable glycemic control, many individuals with diabetes use either carbohydrate counting, carbohydrate exchanges or experience-based estimation of carbohydrate intake as a helpful means to monitor their consumption of carbohydrate at meals or snacks [2]. Besides the amount of carbohydrate, other factors including the nature of starch, the amount of dietary fiber and the type of sugar influence the glycemic response to carbohydrate-containing foods [3134]. For example, eating fresh fruits is superior to a fruit juice with the same amount of carbohydrate. A substantial benefit from these expensive so-called "diabetic" preparations has not been proven. Proper food labeling may help the person with diabetes to make healthy choices from available usual foods. Potential of dietary fiber In many countries, people with diabetes consume only few foods that are rich in dietary fiber and therefore total fiber intake is much lower than recommended (Figure 22. With the relatively low carbohydrate intake in people with diabetes it is not easy to meet recommended quantities of fiber. People with diabetes should be encouraged to choose a variety of fiber-containing foods (vegetables, fruits, wholegrain products) to profit from the proven benefits for glycemic control, insulinemia and serum lipid concentrations [3234,40]. The degree of evidence for recommended carbohydrate and dietary fiber intakes is shown in Tables 22. Adjustment of insulin or insulin secretagogues to carbohydrate intake For people who are treated with insulin or hypoglycemic agents, it is important to match the medication with the amount, type and time of carbohydrate intake to avoid hypoglycemia as well as excessive post-prandial hyperglycemia [1,2]. This advice is now part of many nutrition education programs for people with diabetes who are treated with intensified insulin regimens [18,44]. Self-monitoring of blood glucose offers a helpful means of determining the most appropriate timing of food intake and to make optimal food choices [1]. Individual preferences and the needs of different treatment strategies remain the most important determinants of appropriate meal frequency, portion sizes and carbohydrate intake. Extra carbohydrate may be needed prior to exercise although adjustment of the insulin dosage in those on intensified insulin treatment is often an alternative and preferred choice. Structured training and continuing advice by the diabetes team is needed to enable the people with diabetes to adjust the insulin dosage while considering all three components: blood glucose results, amount and quality of carbohydrate intake as well as the degree of physical activity. Sucrose and other sugars Moderate intake of sucrose (<10% total energy) or other added sugars may be included in the diet of people with diabetes without worsening glycemic control [1,2,25,41]. Although fructose produces a reduction in post-prandial glycemia when it replaces sucrose, this potential benefit is tempered by the fact that fructose may adversely effect serum triglycerides as well as uric acid levels [1,8]. There is no reason to recommend that people with diabetes should avoid naturally occurring fructose. Higher quantities of sugar substitutes may promote undesirable gastrointestinal side effects. Furthermore, it is unlikely that energy-containing sugar substitutes such as sugar alcohols in the amounts likely to be consumed will contribute to an appreciable reduction in total energy intake although they are only partially absorbed from the small intestine [2,8]. Approved non-nutritive sweeteners may also be used by people with diabetes although a special long-term benefit in metabolic control has not been proven. Dietary fat the primary goal concerning dietary fat intake is to restrict the consumption of saturated fatty acids, trans-fats and dietary 351 Part 5 Managing the Patient with Diabetes cholesterol to reduce the risk for vascular disease [1,2,45,46]. Compared with the non-diabetic population, people with diabetes have an increased risk of developing vascular disease.
A common lapse is the omission or reduction of insulin during episodes with impaired well-being and poor appetite symptoms 12 dpo generic thorazine 50 mg on-line. Persistent ketosis should be treated with extra insulin symptoms schizophrenia buy generic thorazine from india, fluid and carbohydrate medicine quinidine buy thorazine line, when necessary medications j-tube buy cheap thorazine 100 mg online. Furthermore, it is very important that the individual patient has ready, 24 hours/ day access to diabetologic expertise, preferably in a specialized diabetes center. In practice this dilemma is mainly ornamental, because diagnostic and therapeutic efforts follow the same principles. Hyperglycemia is caused by a vicious cycle, in which relative insulin deficiency and high levels of stress hormones lead to increased endogenous glucose production and decreased peripheral glucose utilization; hyperglycemia in turn induces hyperosmolality and dehydration, which amplifies the stress hormone response and further impairs insulin secretion and vice versa. Typically, there will be a water deficit of 1020% of body weight together with sodium, chloride and potassium deficits of 510 mmol/kg body weight. Usually 1 L isotonic saline is infused in the first hour but after that slower rehydration is advisable. Hemodynamic performance should be monitored carefully and it should be borne in mind that many of the patients have pre- or coexisting cardiac disease. Hyperglycemic crises in adult patients with diabetes: a consensus statement from the American Diabetes Association. Predictors of intensive care unit and hospital length of stay in diabetic ketoacidosis. Proinflammatory cytokines, markers of cardiovascular risks, oxidative stress, and lipid peroxidation in patients with hyperglycemic crises. The acute splanchnic and peripheral tissue metabolic response to endotoxin in humans. Tumor necrosis factor mimics the metabolic response to acute infection in healthy humans. Intensive insulin therapy exerts antiinflammatory effects in critically ill patients and counteracts the adverse effect of low mannose-binding lectin levels. Tumor necrosis factor impairs insulin action on peripheral glucose disposal and hepatic glucose output. Effects of changes in hydration on protein, glucose and lipid metabolism in man: impact on health. Short-term fasting is a mechanism for the development of euglycemic ketoacidosis during periods of insulin deficiency. Renal amino acid, fat and glucose metabolism in type 1 diabetic and non-diabetic humans: effects of acute insulin withdrawal. Diabetic ketoacidosis in infants, children, and adolescents: a consensus statement from the American Diabetes Association. Different individual susceptibility to microvascular complications have been linked to polymorphisms in the superoxide dismutase 1 gene. Hyperglycemia-induced mitochondrial reactive oxygen species production impairs the neovascular response to ischemia by blunting hypoxia-inducible factor 1 transactivation. Hypertension accelerates microvascular damage by increasing intracellular hyperglycemia through upregulation of the glucose transporter 1. Overview of diabetic complications All forms of diabetes are characterized by hyperglycemia, a relative or absolute lack of insulin action, and the development of diabetes-specific pathology in the retina, renal glomerulus and peripheral nerve. Diabetes is also associated with accelerated atherosclerotic disease affecting arteries that supply the heart, brain and lower extremities. More than 60% of patients with diabetes are affected by neuropathy, which includes distal symmetrical polyneuropathy, mononeuropathies and a variety of autonomic neuropathies causing erectile dysfunction, urinary incontinence, gastroparesis and nocturnal diarrhoea. Diabetic accelerated lower extremity arterial disease in conjunction with neuropathy Textbook of Diabetes, 4th edition. Finally, new blood vessel growth in response to ischemia is impaired in diabetes, resulting in decreased collateral vessel formation in ischemic hearts, and in non-healing foot ulcers. The focus of this chapter is on the microvascular complications comprising retinopathy, nephropathy and peripheral neuropathy. With long-standing disease, there is progressive narrowing and eventual occlusion of vascular lumina, resulting in impaired perfusion, ischemia and dysfunction of the affected tissues.
Quality 100 mg thorazine. Free Fire Only 2 Kill BOOYAH with MS Side GAMER-Garena.
In the setting of an uncomplicated medications xl buy thorazine no prescription, elective procedure to treat stable angina symptoms 9 days past iui purchase genuine thorazine line, the post-procedure waiting period is 1 week medications 44 175 purchase 100mg thorazine free shipping. The waiting period allows for a small threat caused by acute complications at the vascular access site medicine 377 discount 50mg thorazine visa. Decision Maximum certification period - 1 year Recommend to certify if: the driver: · · · Is asymptomatic at examination. Page 98 of 260 Recommend not to certify if: the driver has: · · · Incomplete healing or complication at vascular access site. The driver should obtain: · · Clearance from a cardiovascular specialist who understands the functions and demands of commercial driving. Typical angina symptoms should prompt evaluation with a stress imaging study or repeat angiography. Congenital Heart Disease Heart failure and sudden death are the major causes of death among individuals with congenital heart disease. Due to the complexity of these problems, the Cardiovascular Advisory Panel Guidelines for the Medical Examination of Commercial Motor Drivers recommend that the driver has regular, ongoing followup by a cardiologist knowledgeable in adult congenital heart disease. As a medical examiner, your decision to certify should be based on: · · · · · Anatomic diagnosis. Advances in surgical and medical management are expected to result in an increased number of individuals with congenital heart disease seeking driver certification. Ebstein anomaly is included in the handbook because it is a condition you are likely to encounter in the clinical setting. Ebstein Anomaly Ebstein anomaly is a congenital downward displacement of the tricuspid valve. Adults with a mild form of Ebstein anomaly can remain asymptomatic throughout their lives. Decision Maximum certification - 1 year Recommend to certify if: the driver: · · · · Is asymptomatic. Recommend not to certify if: the driver has a(n): · · · · · Moderate or severe anomaly. Monitoring/Testing Annual cardiovascular re-evaluation should include echocardiography and evaluation by a cardiologist knowledgeable in adult congenital heart disease and who understands the functions and demands of commercial driving. To review the Congenital Heart Disease Recommendation Table, see Appendix D of this handbook. Page 100 of 260 Heart Transplantation Although the number of heart transplant recipients is relatively small, some recipients may wish to be commercial motor vehicle drivers. The major medical concerns for certification of a commercial driver heart recipient are transplant rejection and post-transplant atherosclerosis. Decision Maximum certification period - 6 months Recommend to certify if: the driver: · · · · · Is asymptomatic. Recommend not to certify if: As the medical examiner, you believe that the nature and severity of the medical condition endangers the health and safety of the driver and the public. Monitoring/Testing Monitoring the driver with a heart transplant should include re-evaluation and recertification every 6 months by a cardiovascular specialist who: · · · Is an expert in the fields of cardiology and transplant medicine. Evaluates the possibility of atherosclerosis, the status of the transplant, and the general health of the driver. To review the Heart Transplantation Recommendation Table, see Appendix D of this handbook. Page 101 of 260 Myocardial Disease Myocardial diseases are often progressive and require long-term follow-up. Even so, improved diagnostic testing and treatment can increase the number of drivers with myocardial disease who seek commercial motor vehicle driver certification. Hypertrophic Cardiomyopathy Hypertrophic cardiomyopathy is a complex disease characterized by marked morphologic, genetic, and prognostic heterogeneity. Some individuals experience a benign and stable clinical course, while in others the disease is characterized by progressive symptoms. For some individuals, sudden death is the first definitive manifestation of the disease. Waiting Period If you note an enlarged heart in a driver, you should not certify the driver until evaluation by a cardiovascular specialist who understands the functions and demands of commercial driving to confirm or rule out a diagnosis of hypertrophic cardiomyopathy.
If glucose testing determines that a patient has diabetes medications used for fibromyalgia buy discount thorazine 100 mg line, additional tests may be offered to establish the type medicine rocks state park discount thorazine 50 mg free shipping. People with type 2 diabetes have C-peptide nioxin scalp treatment order 100 mg thorazine otc, which is a byproduct of insulin production medicine administration discount thorazine online american express, but people with type 1 diabetes and latent autoimmune diabetes of adulthood do not nor have a very low level. Autoantibody testing can reveal misguided antibodies present in autoimmune but not metabolic diabetes. Genetic tests can help diagnose conditions such as maturity-onset diabetes of the young and Wolfram syndrome. Other tests, such as thyroid blood tests, may be ordered to find the cause of secondary diabetes. Blood is drawn an hour after the patient drinks a solution containing 50 g of glucose. Treatment options for diabetes Patients who are diagnosed with diabetes usually require regular monitoring by various healthcare providers to manage their condition and reduce the risk of complications. For example, endocrinologists are physicians who specialize in diabetes and other endocrine disorders. In locations where an endocrinologist is not available, an internist or other physician may treat diabetic patients. Diabetes care teams also include certified diabetes educators and registered dietitians. Patients need to see an ophthalmologist and a dentist regularly and may be referred as needed to other specialists such as a podiatrist, athletic trainer, cardiologist, nephrologist (kidney specialist) or neurologist. Diet and exercise are crucial in managing diabetes, especially type 2 diabetes and gestational diabetes. Some patients with metabolic forms of diabetes are able to control their disease using only these lifestyle interventions, which help the body use glucose (blood sugar) and prevent or reduce hyperglycemia. It is also important to avoid smoking, drink enough water to avoid dehydration, and drink alcohol only in moderation and only if approved by the physician. All people with type 1 diabetes and Wolfram syndrome and eventually all people with latent autoimmune diabetes of adulthood require regular insulin therapy to live. Some people with other forms of diabetes, including gestational diabetes, type 2 diabetes, secondary diabetes and maturity-onset diabetes of the young, also are prescribed insulin. Forms of insulin administration include syringe injections, insulin pumps, insulin pens, jet injectors and inhaled insulin. Food and Drug Administration has approved oral diabetes drugs only to treat type 2 diabetes, but physicians sometimes use them to treat other conditions including prediabetes, insulin resistance and polycystic ovarian syndrome. Synthetic amylin is the only drug other than insulin approved to treat type 1 diabetes. Glucagon is a hormone that acts against insulin and can be injected in cases of severe hypoglycemia or insulin shock. Patients with diabetes are often prescribed other medications, including antihypertensive and cholesterol drugs, to treat related conditions. Patients who have or are at high risk for heart conditions may be advised to take low-dose aspirin daily. People with diabetes need to perform glucose monitoring according to the schedule devised by their care team. Some patients use a glucose meter occasionally, but others, especially those using insulin or antidiabetic agents, must test several times a day. In addition to these self-tests, patients will have glycohemoglobin tests or fructosamine tests periodically performed by their physician to assess long-term control of glucose. It is also essential to have regular dilated eye exams and dental care, and periodic tests of kidney function such as microalbuminuria testing and glomerular filtration rate. Samreen 373 Some patients with autoimmune diabetes may be candidates for a pancreas transplant or an experimental islet cell transplant. If successful, these procedures may mean a patient no longer has to take insulin for the lifespan of the transplanted organ or cells (Turner et al. Prevention methods for diabetes There is no known way of preventing autoimmune forms of diabetes (type 1 and latent autoimmune diabetes of adulthood) or genetic conditions such as maturity-onset diabetes of the young and Wolfram syndrome.